II. Significance
Promotes overall blood circulation and helps in the early prevention of complications such as pressure ulcers, urinary tract infections, hypostatic pneumonia, muscle atrophy, joint deformities, etc. It also ensures the achievement of expected outcomes in rehabilitation treatment and nursing care.
III. Classification
•Active (Independent) Transfer: Transfers performed independently by the patient without assistance.
•Assisted Transfer: Transfers performed with the help of therapists or caregivers.
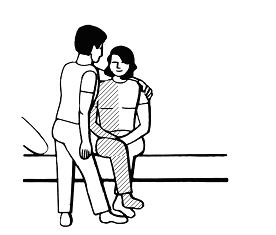
•Passive Transfer: Also known as manual handling, used when the patient is too paralyzed to perform active or assisted transfers. The patient is entirely lifted and moved from one place to another using external force. This includes manual and mechanical handling.
IV. Biomechanical Principles
Successful transfers require good balance and a stable base of support. Both the person transferring and the one being transferred should apply the following biomechanical principles effectively:
1.Keep the object close to the body’s center of gravity.
2.Ensure a wide base of support.
3.Avoid twisting the body while lifting.
4.Adjust foot positioning according to movement direction.
5.Use the strongest body posture.
V. Choosing a Transfer Method
1.If the patient can transfer independently, avoid providing unnecessary help. Use passive transfer only as a last resort.
2.Do not force patients with severe disabilities or cognitive impairments to perform independent transfers.
3.When the transfer distance is too long or transfers are frequent, it is difficult for one person to assist or use a lift every time.
VI. Pre-transfer Training
A. Preparation for Active Transfer
1.Strength and Balance Training
•For turning over: train shoulder girdle and abdominal muscles.
•For moving from lying to sitting: train abdominal and triceps muscles.
•For moving from sitting to standing: train abdominal, quadriceps, calf muscles, and balance.
•For transfers between bed and wheelchair/chair: train upper limb support, lower limb weight-bearing, and balance.
2.Teach Patients Transfer Techniques
•Use momentum from swinging, leverage, and rolling forces to assist in getting up.
B. Preparation for Assisted Transfer
•Patients need some strength and balance. Therapists should follow the active transfer preparation plan for training.
•Explain transfer goals, direction, and methods to gain patient cooperation. Encourage the patient to void before transfer to prevent incontinence.
C. Preparation for Passive Transfer
•Therapists should communicate with the patient to reduce anxiety and resistance, encourage relaxation, and gain cooperation.
VII. Postural Transfer Techniques for Stroke Patients
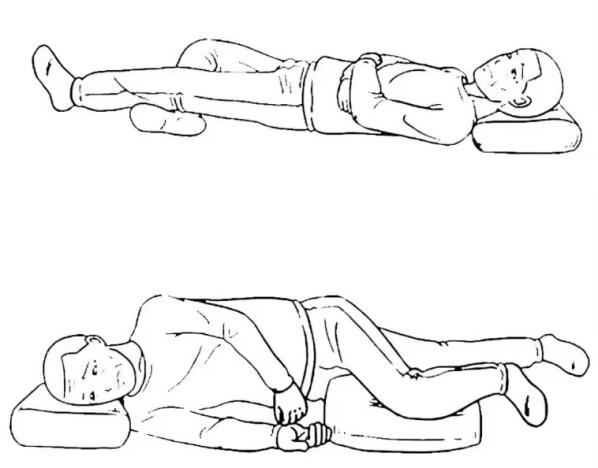
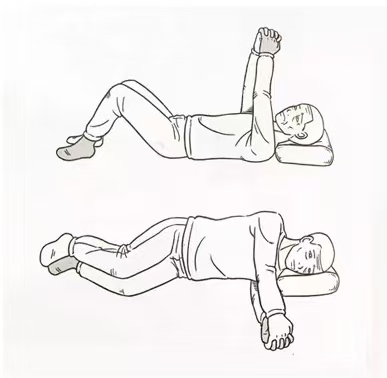
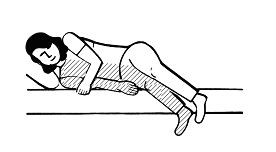
1. Turning Over in Bed
•From supine to affected side: Turn the head to the affected side, abduct the affected arm, bend the sound leg, push against the bed, lift the pelvis, and roll the body.
•From supine to sound side: Place sound foot under affected foot, interlock hands using Bobath method, swing arms to create momentum for the roll.
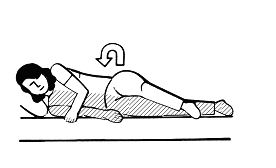
2. Bed Mobility (Lateral and Vertical)
•Side movement (e.g., to the left): Place sound foot under affected foot, interlock hands using Bobath method,lift pelvis using sound limbs, and slide the body sideways.
•Upward movement: Bend the sound leg and elbow, push with foot and elbow, lift pelvis and move upward.
3. From Lying to Bedside Sitting
•From sound side: Interlock hands, move affected leg with sound leg, use sound arm to support and raise the upper body.
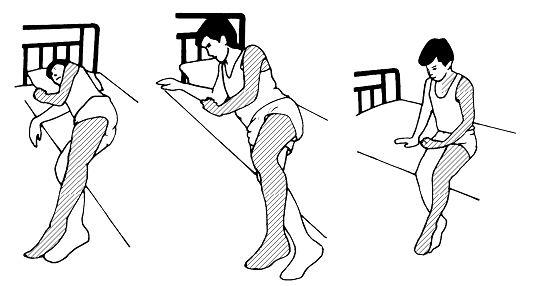
•From affected side: Roll to the side, position affected arm, lean upper body to the side, swing sound leg over, use sound arm for support, sit up.


4. From Sitting to Lying
•From affected side: Place sound hand beside affected hip, lift both legs, lower upper body gradually to lying position.
•From sound side: Place affected leg behind sound leg, lean to sound side, lift legs, lie down using elbow and foot support to adjust body position.
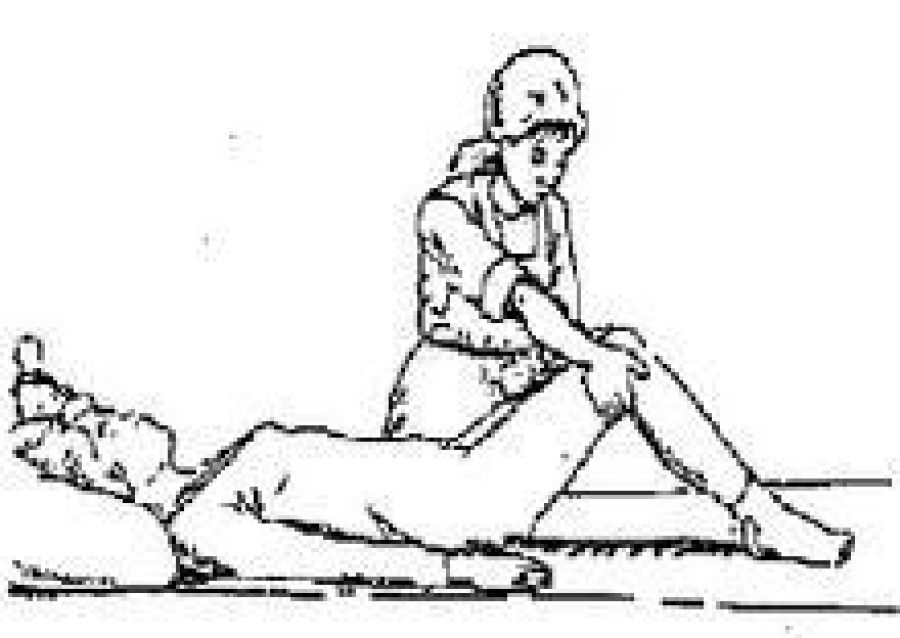
5. Assisted Sitting by Therapist/Caregiver
•Patient lies on side with knees bent.
•Therapist places legs over bed edge, supports upper and lower body, encourages side bend, lifts shoulder, rotates pelvis to seated position.
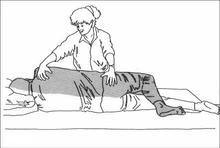
6. Assisted Lying by Therapist/Caregiver
•Patient sits at bed edge, affected hand on thigh, therapist supports neck/shoulder and legs, helps lift legs, adjusts patient’s position on bed.

7. Sitting Transfer in Bed
•Bend both legs, use sound hand to support the body during movement.
8. Independent Transfer from Bed to Wheelchair
•Position wheelchair at 45° on sound side, lock brakes, remove footplate/armrest.
•Support with sound hand on wheelchair armrest, push with feet, lift pelvis, rotate to sit in wheelchair.
9. Standing Up and Sitting Down
A.From sitting to standing:
•Feet shoulder-width apart, heels behind knees, affected foot slightly back.
•interlock hands using Bobath method, extend arms, lean forward, shift weight, stand up slowly.
B.From standing to sitting:
•Back against bed, feet even,interlock hands using Bobath method.
•Lean forward, keep spine straight, shift weight back, bend knees/hips, slowly sit down.
10. Notes for Chair/Wheelchair Transfers
•Chair should be firm, stable, and high for easier standing.
•Prefer chairs with armrests.
•Lock wheelchair brakes and remove footrests before transfer.